Updated June 7, 2024
Management of stage I and II ovarian cancer aims to maximize survival while minimizing treatment-related morbidity [27]. For stage I ovarian cancer, the cornerstone is surgical staging and cytoreduction (see section 3.2). Some patients with stage IA or IB disease may not require adjuvant therapy, whereas those with high-grade tumours (e.g., HGSC) or stage IC disease typically receive adjuvant chemotherapy, commonly a platinum-based regimen such as carboplatin and paclitaxel (see section 5, Subtype specific management).
Stage II ovarian cancer management also begins with optimal cytoreductive surgery. Due to the higher risk of residual disease and metastasis, adjuvant chemotherapy is indicated for all patients with stage II disease. Standard adjuvant chemotherapy involves six cycles of platinum and taxane agents, mirroring the regimen used for advanced-stage disease (see section 5, Subtype specific management).
The inclusion of targeted therapies, such as PARP inhibitors, is under investigation for early-stage disease but is not standard and not approved in Canada or any other jurisdiction.
Management of stage III and IV ovarian cancer, characterized by extensive peritoneal dissemination or distant metastasis, focuses on maximizing surgical cytoreduction and systemic therapy to improve survival outcomes. Post-surgical management includes platinum-based chemotherapy, typically combining carboplatin and paclitaxel for six cycles and often a decision about maintenance therapy (see section 4.3 Maintenance therapy).
Pre-operative chemotherapy is appropriate for selected patients with advanced and biopsy-proven ovarian/fallopian tube/primary peritoneal malignancy who are not appropriate for immediate maximal debulking. The decision to delay surgery should be made following consultation with a gynecologic oncologist, in a multidisciplinary team setting (see sections 3 Surgery and 3.4 Delayed Primary Debulking). We recommend routine monitoring of CA125 or other relevant marker with each cycle, and that patients are referred back to Gynecologic Oncology (surgeon) after 2-3 cycles to be evaluated for delayed debulking surgery and to arrange timely care. A CT chest/abdomen/pelvis should be performed prior to the assessment by the Gynecologic Oncologist to determine response to chemotherapy and the distribution of disease. If the chemotherapy has reduced the burden of disease, the distribution is accessible, and the patient’s performance status is satisfactory, then surgery is usually planned post cycle 3 or 4. If there is progressive disease on pre-operative chemotherapy, there is generally no role for surgery, except for bowel or ureteric obstruction. Generally, total number of chemotherapy cycles is 6. Historically, at least 2 additional cycles were given after delayed primary debulking, thus sometimes exceeding 6 cycles, however, currently, with the use of maintenance therapy (see section 4.3 Maintenance therapy) chemotherapy treatment is often completed with cycle 6. Ultimately, the number and timing of cycles will depend on disease status, patient preference and physician preference. There are no data to demonstrate improved patient outcomes beyond 6 cycles of standard chemotherapy.
Timing of initiation of post-operative chemotherapy: Treatment should be started as soon as it is felt safe to do so after surgery, with the goal of completing 6 cycles of chemotherapy in total, when possible. For most patients who have an uncomplicated post-operative course, this is often safe and feasible within 14-21 days of the operation. Early treatment initiation prevents the re-accumulation of ascites and is not associated with delays in surgical healing or post-operative complications. Randomized data are not available to define the optimal interval of time for treatment initiation, but retrospective analyses show worse prognosis when treatment delays are excessive.
Maintenance therapy has shown to improve progression-free survival (PFS) and in some cases impact overall survival and is often recommended for stage III and IV disease - see below (section 4.3 Maintenance therapy).
In recurrent disease, treatment is guided by the platinum-free interval, with platinum-sensitive recurrences favouring re-treatment with platinum-based regimens, potentially combined with PARP inhibitors or bevacizumab. Ongoing research is focused on optimizing therapeutic combinations and sequencing to enhance overall survival and quality of life.
Patients with stage I and II high-grade EOC are not eligible for maintenance therapy after the completion of adjuvant chemotherapy.
Maintenance therapy in the first-line treatment setting of advanced-stage ovarian cancer (stage III/IV) predominantly involves the use of PARP inhibitors or bevacizumab which have shown efficacy in improving patient outcomes. PARP inhibitors, such as olaparib and niraparib, leverage synthetic lethality in tumours with homologous recombination deficiencies (HRD), including BRCA1/2 mutations. The SOLO1 trial revealed that maintenance olaparib significantly enhanced PFS and improves 7-year overall survival in cases with BRCA mutations (germline or tumour/somatic) post-response to platinum-based chemotherapy [28]. Similarly, the PRIMA trial established niraparib’s impact on PFS in BRCA1/2 mutated ,HRD-positive and BRCA-wild-type populations, and even in HRD-negative populations [29]. However, recent data demonstrate that maintenance niraparib made no improvement on OS in any molecular subgroup [30]. The reasons for this are unclear and may be multiple. One hypothesis is that high rates of treatment with PARP inhibitors in subsequent lines of therapy may have confounded the results. Both olaparib and niraparib are approved for use in Canada and are available in BC.
Bevacizumab is an anti-angiogenic agent that inhibits vascular endothelial growth factor (VEGF), thus curtailing tumour angiogenesis. The GOG-0218 and ICON7 trials demonstrated that adding bevacizumab to chemotherapy, followed by maintenance bevacizumab, significantly improved PFS in newly diagnosed advanced ovarian cancer [31-33]. ICON7 identified a high-risk population that benefited most from the addition of bevacizumab (i.e., stage IV disease, sub-optimally debulked patients with visible residual disease and patient who were never felt to be candidates for surgery due to disease distribution or other factors). Bevacizumab is approved for use by Health Canada for the high-risk population.
Choice of first-line maintenance therapy: The optimal choice of maintenance therapy for advanced stage (stage III/IV) high-grade ovarian cancer is not known in each case [35]. The decision requires review with an oncologist to integrate treatment, biomarker and patient factors to personalize care.
The following principles may be used to guide decision making:
Table 3: First-line Advanced EOC - Maintenance Therapy Approach in Patients Treated with Pre-Operative Chemotherapy
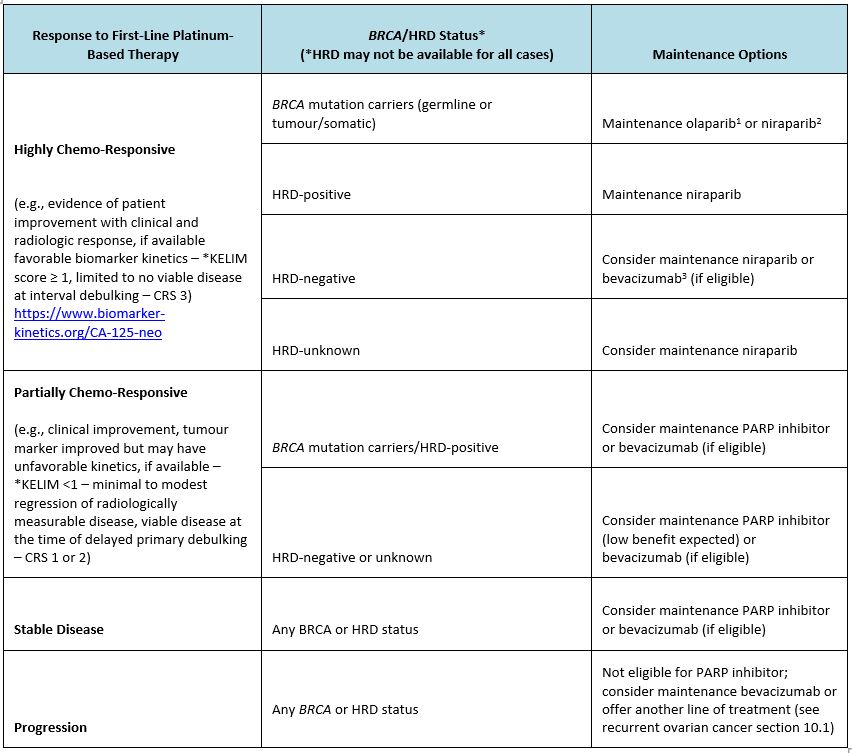
Note: The final treatment decision should be made in consultation with an oncologist, considering individual patient factors and eligibility criteria.
*For patients with stage III or IV high grade serous ovarian carcinomas treated with pre-operative carboplatin – paclitaxel regimen (every 3 weeks or weekly) in first-line setting. A minimum of 3 values of CA-125 within 100 days are required, starting with Cycle 1 day 1 .
https://www.biomarker-kinetics.org/CA-125-neo
1Olaparib GOOVFOLAM Protocol up to 2 yrs of therapy (patients with partial response who are still deriving benefit from olaparib at 2 years may be considered for extension of therapy).
2Niraparib GOOVFNIRM Protocol up to 3 yrs of therapy.
3Bevacizumab GOOVCATB Protocol up a maximum of 17 total doses of bevacizumab.
Table 4: First-line Advanced EOC - Maintenance Therapy Approach in Patients Treated with Post-Operative Chemotherapy Note: The final treatment decision should be made in consultation with an oncologist, considering individual patient factors and eligibility criteria.
*For patients with stage III or IV high grade serous ovarian carcinomas treated with adjuvant carboplatin – paclitaxel regimen (every 3 weeks or weekly) in first-line setting, after primary debulking surgery. A minimum of 3 values of CA-125 within 100 days are required, starting with Cycle 1 day 1.
https://www.biomarker-kinetics.org/CA-125 1Olaparib GOOVFOLAM Protocol up to 2 yrs of therapy (patients with partial response who are still deriving benefit from olaparib at 2 years may be considered for extension of therapy).
2Niraparib GOOVFNIRM Protocol up to 3 yrs of therapy.
3Bevacizumab GOOVCATB Protocol up a maximum of 17 total doses of bevacizumab.
Most patients being diagnosed with EOC today will have been exposed to a PARP inhibitor during first-line therapy. However, some patients (e.g., initially diagnosed with stage I or II disease, or had first-line treatment before maintenance therapy for advanced disease was routinely available) may have disease recurrence and for them, maintenance therapy may be considered once chemotherapy is completed.
The pivotal NOVA trial demonstrated that niraparib significantly prolonged progression-free survival (PFS) in both BRCA-mutated and non-BRCA patients with recurrent platinum-sensitive (recurrence > 6 months from the time of the last platinum-based therapy) and platinum-responsive (evidence of response to the last line of platinum-based therapy) ovarian cancer [35]. There was no improvement in overall survival The SOLO2/ENGOT-Ov21 trial further established the efficacy of olaparib in BRCA-mutated recurrent ovarian cancer, showing a significant improvement in PFS and overall survival (OS) compared to placebo [36].
27. Colombo, N., Sessa, C., Du Bois, A., Ledermann, J., McCluggage, W. G., McNeish, I., ... & Vergote, I. (2019). ESMO-ESGO consensus conference recommendations on ovarian cancer: pathology and molecular biology, early and advanced stages, borderline tumours and recurrent disease. Annals of Oncology, 30(5), 672-705.
28. Moore K., et al. Maintenance Olaparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N Engl J Med. 2018 Dec 27;379(26):2495-2505. doi: 10.1056/NEJMoa1810858. Epub 2018 Oct 21. PMID: 30345884.
29. González-Martín A., at al.; PRIMA/ENGOT-OV26/GOG-3012 Investigators. Niraparib in Patients with Newly Diagnosed Advanced Ovarian Cancer. N. Engl. J. Med. 2019 Dec 19;381(25):2391-2402. doi: 10.1056/NEJMoa1910962. Epub 2019 Sep 28. PMID: 31562799.
30. Monk B.J., Barretina-Ginesta M.P., Pothuri B., Vergote I., Graybill W., Mirza M.R., McCormick C.C., Lorusso D., Moore R.G., Freyer G., O'Cearbhaill R.E., Heitz F., O'Malley D.M., Redondo A., Shahin M.S., Vulsteke C., Bradley W.H., Haslund C.A., Chase D.M., Pisano C., Holman L.L., Pérez M.J.R., DiSilvestro P., Gaba L., Herzog T.J., Bruchim I., Compton N., Shtessel L., Malinowska I.A., González-Martín A. Niraparib first-line maintenance therapy in patients with newly diagnosed advanced ovarian cancer: final overall survival results from the PRIMA/ENGOT-OV26/GOG-3012 trial. Ann. Oncol. 2024 Sep 14:S0923-7534(24)03762-1. doi: 10.1016/j.annonc.2024.08.2241. Epub ahead of print. PMID: 39284381.
31. Burger, R. A., Brady, M. F., Bookman, M. A., Fleming, G. F., Monk, B. J., Huang, H., ... & Liang, S. X. (2011). Incorporation of bevacizumab in the primary treatment of ovarian cancer. New England Journal of Medicine, 365(26), 2473-2483.
32. Oza A.M., et al. Standard chemotherapy with or without bevacizumab for women with newly diagnosed ovarian cancer (ICON7): overall survival results of a phase 3 randomised trial. Lancet Oncol. 2015 Aug;16(8):928-36. doi: 10.1016/S1470-2045(15)00086-8. Epub 2015 Jun 23. PMID: 26115797; PMCID: PMC4648090.
33. Perren T.J., et al.. A phase 3 trial of bevacizumab in ovarian cancer. N. Engl. J. Med. 2011 Dec 29;365(26):2484-96. doi: 10.1056/NEJMoa1103799. Erratum in: N. Engl. J. Med. 2012 Jan 19;366(3):284. PMID: 22204725.
34. Banerjee S., Gonzalez-Martin A., Harter P., Lorusso D., Moore K.N., Oaknin A., Ray-Coquard I. First-line PARP inhibitors in ovarian cancer: summary of an ESMO Open - Cancer Horizons round-table discussion. ESMO Open. 2020 Nov;5(6):e001110. doi: 10.1136/esmoopen-2020-001110. PMID: 33310779; PMCID: PMC7783599.
35. Mirza M.R., et al.. Niraparib Maintenance Therapy in Platinum-Sensitive, Recurrent Ovarian Cancer. N. Engl. J. Med. 2016 Dec 1;375(22):2154-2164. doi: 10.1056/NEJMoa1611310. Epub 2016 Oct 7. PMID: 27717299.
36. Pujade-Lauraine E., et al.. Olaparib tablets as maintenance therapy in patients with platinum-sensitive, relapsed ovarian cancer and a BRCA1/2 mutation (SOLO2/ENGOT-Ov21): a double-blind, randomised, placebo-controlled, phase 3 trial. Lancet Oncol. 2017 Sep;18(9):1274-1284. doi: 10.1016/S1470-2045(17)30469-2. Epub 2017 Jul 25. Erratum in: Lancet Oncol. 2017 Sep;18(9):e510. doi: 10.1016/S1470-2045(17)30639-3. PMID: 28754483.

